EEG
Snimanje EEG-a
Standardni sustav postavljanja i označavanja elektroda 10-20 (21 elektroda). Neparni brojevi lijevo, parni desno; F (frontalno), P (parijetalno), C (centralno), O (okcipitalno).
Montaže
- longitudinalna bipolarna
- longitudinalna transverzalna
- montaža prema referentnoj točci
Frekvencijske karakteristike EEG-a
Delta-ritam
- frekvencija: 0,5 – 3,5 Hz | amplituda: 20 – 200 µV
- kod zdravih osoba u dubokom snu; kod budne osobe – pokazatelj patologije SŽŠ-a.
Theta-ritam
- frekvencija: 4 – 7 Hz; amplituda 20 – 100 µV
- češće kod djece nego odraslih; kod odraslih se javlja u stanju pospanosti i laganog sna, također može biti pokazatelj patologije SŽŠ-a.
Alfa-ritam
- frekvencija: 8 – 12 Hz | amplituda: 20 – 60 µV
- tipično okcipitalno, u stanju relaksacije (mirno sjedenje zatvorenih očiju)
Beta-ritam
- frekvencija: 12 – 30 Hz | amplituda: 2 – 20 µV
- stanje normalne, zdrave budnosti, povećane koncentracije te intenzivne mentalne aktivnosti
ES EEG
- Glavni pojmovi 1 - lokalizacija uzorka
- Glavni pojmovi 2
- morfologija svakog uzorka kao periodička izbijanja, ritmičku delta aktivnost ili šiljak val kompleks
- modifikatori - prevalencija, trajanje, broj faza, oštrina vala amplituda, polarnost, induciranje stimulusima, razvoj/fluktuiranje, dodatni uzorci
Najvažniji uzorci:
- lateralizirajuća periodička izbijanja (LPD) - stereotipna repetitivna visokovoltažna (100 - 300 μV) izbijanja u regularnim intervalima koja involviraju jednu hemisferu, frekvencije ≤ 1 Hz
- ritmička delta aktivnost (RDA) - ritmičko ponavljanje valova frekvencije ≤ 4 Hz, realtivno unimorfne morfologije i trajanja
- bilateralna neovisna lateralizirajuća periodička izbijanja (BIPD) - stereotipna repetitivna izbijanja u regularnim intervalima koja involviraju obje hemisfere
- generalizirana periodička izbijanja (GPD) - difuzna i sinkrona periodička kratka izbijanja šiljaka, polišiljaka ili šiljak-val kompleksa iznad obje hemisfere
- intermitentna ritmička delta aktivost (IRDA) - intermitentna ritmička delta aktivnost predominantno iznad frontalnih (FIRDA) ili posteriornih regija (OIRDA)
- lateralizirajuća delta aktivnost (LRDA) - repetitivni valovi u jednoj hemisferi s relativno uniformnom morfologijom i trajanjem, frekvencije ≤ 3 Hz (slična LPD, ali brža)
- trifazički valovi - kontinuirana 1-2 Hz generalizirana periodička izbijanja s trifazičkom morfologijom
Post-CPR EEG
Post-anoxic EEG findings can be divided into six categories.
- Isoelectric EEG
- EEG with voltage lower than 20 mV
- Burst suppression EEG with a subcategory of burst suppression with identical bursts
- Epileptiform EEG including status epilepticus and periodic discharges
- Continuous activity less than 8 Hz
- Continuous activity equal to or greater than 8 Hz
EEG findings consistently associated with a poor outcome when seen 24 hours after an arrest are isoelectric EEG, low voltage EEG, and burst suppression (specifically burst suppression with identical bursts), as well as the absence of EEG reactivity.
- isoelectric EEG and low voltage EEG are associated with diffuse cortical injury and brain death.
- burst suppression is defined as high amplitude activity with at least four phases and lasting at least 500ms with alternating low or absent EEG activity. Specific observations related to burst suppression are that longer suppressions have generally been associated with poor outcomes in the setting of post anoxic coma. Burst suppression with identical bursts has been found to be distinct form burst suppression due to other etiologies including pharmacologically induced burst suppression.
- reactivity is defined as any change in frequency or amplitude of an EEG following a stimulus. The absence of reactivity in multiple studies has been invariably associated with poor outcome, though the timing of this finding in relation to the anoxic injury is not well clarified. These findings have less or unknown significance prior to 24 hours post event.
- EEG findings consistently associated with more favorable outcomes are progressive return of physiologic rhythms within 12 hours of the arrest, reactive EEG, and the absence of malignant patterns.
While EEG findings consistent with patterns on either end of the prognostic spectrum (i.e. relatively good or very poor) are helpful, indeterminate patterns remain common and complicate bedside prognosis. These include generalized periodic discharges, lateralized periodic discharges, generalized rhythmic delta activity, and lateralized rhythmic delta activity.
EEG faze sna
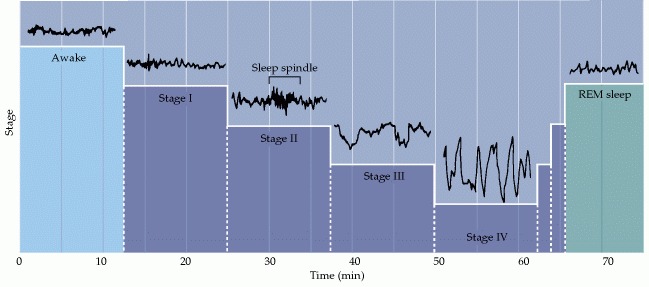
EEG recordings during the first hour of sleep.
- The waking state with the eyes open is characterized by high-frequency (15–60 Hz), low-amplitude activity (~30 μV) activity - beta activity.
- Descent into stage I non-REM sleep is characterized by decreasing EEG frequency (4–8 Hz) and increasing amplitude (50–100 μV) - theta waves.
- Descent into stage II non-REM sleep is characterized by 10–15 Hz oscillations (50–150 μV) called spindles, which occur periodically and last for a few seconds.
- Stage III non-REM sleep is characterized by slower waves at 2–4 Hz (100–150 μV).
- Stage IV sleep is defined by slow waves (also called delta waves) at 0.5–2 Hz (100–200 μV). After reaching this level of deep sleep, the sequence reverses itself and a period of rapid eye movement sleep, or REM sleep, ensues.
- REM sleep is characterized by low-voltage, high-frequency activity similar to the EEG activity of individuals who are awake.
Humans descend into sleep in stages that succeed each other over the first hour or so after retiring. These characteristic stages are defined primarily by electroencephalographic criteria. Initially, during “drowsiness,” the frequency spectrum is shifted toward lower values and the amplitude of the cortical waves slightly increases. This drowsy period, called stage I sleep, eventually gives way to light or stage II sleep, which is characterized by a further decrease in the frequency of the EEG waves and an increase in their amplitude, together with intermittent high-frequency spike clusters called sleep spindles. Sleep spindles are periodic bursts of activity at about 10–12 Hz that generally last 1 or 2 seconds and arise as a result of interactions between thalamic and cortical neurons. In stage III sleep, which represents moderate to deep sleep, the number of spindles decreases, whereas the amplitude of low-frequency waves increases still more. In the deepest level of sleep, stage IV sleep, the predominant EEG activity consists of low frequency (1–4 Hz), high-amplitude fluctuations called delta waves, the characteristic slow waves for which this phase of sleep is named. The entire sequence from drowsiness to deep stage IV sleep usually takes about an hour.
These four sleep stages are called non-rapid eye movement (non-REM) sleep, and its most prominent feature is the slow-wave (stage IV) sleep. It is most difficult to awaken people from slow-wave sleep - it is considered to be the deepest stage of sleep. Following a period of slow-wave sleep EEG recordings show that the stages of sleep reverse to reach rapid eye movement (REM) sleep. In REM sleep, the EEG recordings are remarkably similar to that of the awake state. After about 10 minutes in REM sleep, the brain typically cycles back through the non-REM sleep stages. Slow-wave sleep usually occurs again in the second period of this continual cycling, but not during the rest of the night. On average, four additional periods of REM sleep occur, each having longer durations.
The typical 8 hours of sleep experienced each night comprise several cycles that alternate between non-REM and REM sleep, the brain being quite active during much of this supposedly dormant, restful time. For reasons that are not clear, the amount of REM sleep each day decreases from about 8 hours at birth to 2 hours at 20 years to only about 45 minutes at 70 years of age.