Stroke guidelines
IVT in patients previously treated with antiplatelet aggregation therapy
- Monotherapy: aspirin/clopidogrel/aspirin+dipyridamole/ticagrelor: no restrictions
- Dual therapy: aspirin+clopidogrel: no restrictions; other combinations: consider IVT carefully
- Monotherapy or combination therapy with prasugrel: consider IVT carefully
- Triple therapies: no IVT
Stroke Unit treatment
Cardiovascular monitoring:
- BP upper limits during the early phase:
- ≤ 185/105 mmHg after IVT
- ≤ 140/95 mmHg after successful EVT (TICI 2b or 3), otherwise ≤ 185/105 mmHg
- ≤ 220/110 mmHg in conservatively treated patients
- BP lower limit: only in selected cases in case of hypoperfusion/symptom worsening with drop of BP => to increase BP: only temporary administration of a limited volume of infusion solution (max. 500 ml); in other cases use vasopressors (e.g. Noradrenaline)
- Tachycardia > 100 bpm => usually beta blockers; in case of tachycardic atrial fibrillation consider adding digoxin
- Frequent ventricular extrasystole => magnesium 2 g i.v.
- Bursts of ventricular extrasystole (more than 3 beats): usually beta blocker + magnesium; ≥10 beats or polymorph or >120/min or clinically symptomatic => consultation with cardiologist
- Bradycardia: during sleep in asymptomatic patients, usually up to 35 bpm is tolerable
- Pause > 3 seconds => consultation with cardiologist
Respiration: target Biox ≥ 92; screening for sleep apnoea
- If > 4l O2/min is necessary or respiration frequency > 20 => clinical examination, arterial blood gas analysis, chest X-ray (pulmonary embolism? cardiac failure? pneumonia?)
- If respiration frequency > 25–30 there may be a danger of respiratory exhaustion
Body temperature: ≥ 38° -> antipyretics (1st choice paracetamol) + 2x2 blood cultures, empirical/causal treatment
Clinical general medical evaluations: cardiac compensation, lungs, abdomen to be checked daily
Prescription of medication:
- Do not prescribe antiplatelet aggregation therapy after IVT/i.a Urokinase before exclusion of haemorrhage in control CT/MRI after 24h
- General cardiac premedication should be continued, with potential reduction of dose (WARNING cardiac failure/rebound tachycardia after stop)
- Stop any antihypertensive medication in the case of haemodynamic stroke
Laboratory controls: (24h after IVT/EVT)
- Hb, Lc, Tc, CRP, glucose, Na, K, creatinine, INR - hs-Troponin T and ECG after 1 h if initially abnormal
- Anaemia: transfusion if Hb < 90 g/l - Tc daily under heparin therapy; further laboratory examinations individually determined
Neuroradiological control:
- 24h after IVT/EVT, MRI (or CT), including MRA (CTA) except in patients with severe renal insufficiency
- In case of neurological deterioration immediately
Swallowing: in case of dysphagia, reduced consciousness , facial palsy or relevant neuropsychological deficits: swallowing test (GUSS: Gugging Swallowing Screen)
Nutrition and fluid balance:
- Daily fluid intake requirement: 30–35 ml/kg body weight
- Daily energy demand: 35 kcal x body weight
- If sufficient oral energy supply cannot be given within 3 days after stroke: enteral feeding via nasogastric tube with high caloric fibrous enteral feeding as bolus application 3–4x/d; control of electrolytes (incl. magnesium and phosphate)
- If fasting period > 7 days: delayed feeding (WARNING refeeding syndrome)
DD Neurological deterioration
- Reinfarction
- Infarct localization: e.g. secondary deterioration more frequent in internal capsula or pontine infarctions
- Haemodynamic: BP associated? Associated with mobilization?
- Bleeding
- Rising ICP
- Epileptic seizure
- Infection
- Sedation
- Psychogenic and other less frequent causes
Alteplase-associated ICH
In the case of symptomatic ICH or neurological deterioration within 24 after Alteplase administration:
- → Stop Alteplase
- → Blood tests: thrombocytes, INR, aPTT, fibrinogen, type and cross-match
- → CT; in case of bleeding:
- → Fibrinogen (Haemocomplettan P) or Prothrombin complex concentrate (involve haematology)
- → Tranexamic acid (Tranexam OrPha) i.v. 1000 mg, apply over 10min
- → BP aim ≤ 140/90 mmHg
Malignant infarcts
General
- Usually 30° supine position
- BP aim: MAP > 85 mmHg, sys. < 220 mmHg
- In case of imminent craniectomy: stop antiplatelet therapy
- Pneumatic compression stockings for prevention of deep vein thrombosis
- Consider as emergency medication until craniectomy:
- mannitol/hypertonic saline solution (dosage control of mannitol via osmotic gap, hypertonic saline solution via Na and osmolality)
- Hyperventilation
Decompressive craniectomy
- Craniectomy if possible within 24–48 h and before relevant neurological deterioration
- Critical phase with risk for neurological deterioration: 24–96 h (rarely up to as late as 10 d)
- Signs of rising ICP: decreasing consciousness, disturbance of pupillomotor function usually with dilatation in case of supratentorial swelling, and miosis in case of infratentorial swelling, increasing paresis, new ipsilateral paresis, pathological breathing pattern, rhythmic disorders
- Possible practical approach:
- general actions see above
- frequent clinical control and early CT control (e.g. 12 h after stroke) in case of infarct >2/3 middle cerebral artery territory or larger infratentorial stroke (e.g. complete PICA infarct or larger)
- aim: preventive decompression! Rescue therapy only in exceptional circumstances and probably associated with worse outcome
Malignant infarctions of the middle cerebral artery territory
Predictors for malignant infarction: young patient, persistent vessel occlusion, early midline shift ≥ 4mm, critical infarct volume dependent upon age/atrophy but >>80 ml or >1/2 media territory, additional infarction in anterior or posterior territory
Indications for craniectomy
- Usually < 60 years, individually consider also in older patients
- Symptom onset within the past 48 h (in exceptional cases this may be longer)
- Infarction of at least half of the middle cerebral artery territory
- Consent of patient or family
- Indication independent from affected hemisphere (dominant vs. non-dominant)
Contraindications
- Bilateral fixed pupils and coma
- More than 3 of the following unfavourable prognostic factors:
- age >50 years
- infarction extends beyond the middle cerebral artery territory
- unilateral dilated pupil
- GCS <8
- Severe comorbidity; severe preexisting disability
Malignant cerebellar infarctions
Predictors for malignant infarction: young patient, persistent vessel occlusion, bilateral infarction, the size has less predictive value because small infarcts may induce large oedema
Indications for craniectomy
- Larger infratentorial ischaemia (e.g. complete PICA stroke)
- Imaging shows space-occupying infarction with progression in short term follow-up imaging
- Consent of patient or family
Contraindications
- Clinical or imaging signs of severe irreversible brainstem damage
- Severe comorbidity, severe preexisting disability
Agitation/delirium
Diagnostic criteria ICD-10
- Reduced attention → reduced perception of evironment
- Disordered thinking, manifest through
- limited short-term memory
- Disorientation (place, time, person)
- Psychomotor abnormalities, of the following:
- rapid, unpredictable change from hypo- to hyperactivity
- extended reaction times
- changed speaking speed
- startle reaction
- Sleep abnormalities, at least one of the following:
- insomnia with or without daytime sleepiness
- symptoms worse at night
- nightmares (can sometimes continue into the day as hallucinations/illusional misjudgement)
- acute onset and fluctuating throughout the day
- Evidence of an organic brain or systemic disease (partly) responsible
Symptomatic therapy
In case of alcohol withdrawal delirium, 1st choice is benzodiazepines, otherwise use the following scheme:
Level 1:
- Quetiapine 12.5 mg stepwise (maximal dose 800 mg/d)
- or/and Risperidone 2×0.5 mg/d (maximal dose 16 mg/d)
- or exceptional Haloperidol 0.5–1 mg stepwise (maximal dose 60 mg/d)
Level 2:
- Diazepam 5 mg stepwise i.v. (increase up to 10 mg stepwise is possible)
- or Midazolam: 2.5–5 mg as bolus (maximal dose 10 mg);
then, if necessary, 2–5 mg/h perfusion therapy (maximal dose 10 mg/h) – antidote: Flumazenil
Level 3: Clonidine: 25–50 g as bolus, then 25–150 g/h perfusion therapy (maximal dose 150 g/h)
Level 4: Dexmedetomidine or Propofol with perfusor in ICU
Special case, delirium in patients with stroke and Parkinsons disease
- Quetiapine 25–100 mg p.o., max. 300 mg/d
- Clozapine 6.25–12.5 mg, max. 100 mg/d; 2/3 of the dose at night, 1/3 throughout the day
Special case, delirium in patients with stroke and alcohol withdrawal → Primarily benzodiazepines + thiamine substitution
TIA and minor stroke
- Pathological definition of TIA: transient neurological deficit without diffusion restriction in MRI
- Time-dependent definition of TIA: transient neurological deficits of < 24 h duration
- Definition of minor stroke: NIHSS ≤ 4, symptoms stable or improving
DD TIA, seizure, migraine aura
- TIA: usually negative symptoms, spread of symptoms usually fast
- Seizure: usually positive symptoms, spread of symptoms fast
- Migraine aura: usually postive symptoms, spread of symptoms over minutes
Frequent causes
Cardioembolism/paradoxical embolism
- Atrial fibrillation/flutter
- Myocardial infarction
- Other dysrhythmia (e.g. sick sinus syndrome, silent atrium)
- Valve disease
- Endocarditis
Paradox embolic
- PFO/ASD
- pulmonary shunt
Large artery disease
- Arterio-arterial embolism
- Aortic arch embolism
- Non atherothrombotic vasculopathy (e.g. FMD)
Other causes
- Dissection (incl. aorta)
- Small artery disease (lacunar <1.5 cm + BG)
- Vasculitis
- Chronic infection (in particular HIV, Hep B/C, syphilis)
- Factor V Leiden/thrombophilia/anti-cardiolipin/lupus anticoagulant
- Acute coagulation disorders (especially DIC)
- Coagulation disorders associated with tumour
- Fabry disease
- Sickle cell disease/other haemolytic crises
- Polyglobulia/thrombocytosis
- Drugs
- Iatrogenic (e.g. periinterventional)
Etiological DD according to results
History & Physical examination
- Circumstance at onset (e.g., Valsalva?)
- Positive familial history with onset < 40 years (Fabry disease, coagulopathy)
- < 50 years, previous art/ven thrombosis, abortion (anti-phospholipid syndrome), Fabry disease
- Throat/neck/eye pain, trauma (dissection ICA/VA)
- Headache (vasculitis), thunderclap headache (reversible vasoconstriction syndrome)
- Heart murmurs (endocarditis, valvular calcification)
- Angina pectoris (acute or in the past)
- Acute chest/back pain (aortic dissection!, coronary syndrome)
- Peripheral vascular examination incl. BP-difference left-right (aortic dissection)
- Skin lesions (septic emboli, Fabry: angiokeratoma, Sneddon: livedo racemosa)
- Vision disturbance + hearing disturbance (Susac‘s syndrome => corpus callosum affected?)
- Signs of systemic rheumatic disease
- B symptoms
- Acute or chronic infection
Lab
- Signs of infection: Infection-associated coagulopathy? Malignancy? Endocarditis? Systemic disease?
- Thrombocytopenia/Thrombocytosis, Leucocytopathology: haematological disease?
- Anaemia: Malignancy? Sickle cell anaemia?
- D-Dimer
- < 500: more likely arterio-arterial, aorto-embolic, microvascular
- 500–3000: associated with atrial fibrillation
- > 3000: Malignancy? Coagulopathy?
MRI
- > 2 vessel territories affected: cardio-embolic, aorto-embolic, coaguloathy (D-Dimer? Fibrinogen?), paradox embolic, vasculitis
- 1 vessel territory with multipe ischaemia: arterio-arterial (Plaque-MRI?)
Diagnostic work-up (modified)
- imaging: CT / CTA / MR / MRA
- neurovascular ultrasound
- 12-lead ECG
- Long-term ECG
- TEE or TTE
- Routine laboratory testing: Na, K, CRP, ESR, glucose, HbA1c, creatine, urea, CK, AST, ALT, GGT, TSH, complete blood count, coagulation state, blood lipids
- < 50 years: additionally lupus anticoagulant, anti-cardiolipin (IgG+M, not A!), anti-b2GPI (IgG+M, not A!) (if elevated after 3 months, repeat).
Dissections
- According to current data the preventive effects of aspirin and OAC are probably comparable
- In cases of higher grade extracranial stenosis due to dissection or occlusions without large infarction or haemorrhagic transformations, consider OAC/therapeutic heparinizaton followed by OAC
- OAC is generally contraindicated in the case of intradural dissections or dissections extending intradurally (elevated risk for SAH)
- In the case of uncertain diagnosis with fat-suppressed T1 sequences in MRI: extend to regular diagnostic work-up after stroke
- Off-label use of DOAC can be considered in individual cases if OAC cannot be adjusted
PFO
Occlusion of PFO in the case of cryptogenic stroke (at least TTE/TEE and one 7-day ECG negative) and/or RoPE score < 5in patients >60 years. The decision should be made individually and RoPE score serves as orientation.
Consider circumstances that may facilitate paradoxical embolism (e.g. deep vein thrombosis, onset of neurological symptoms after Valsalva manoeuvre, co-existence of atrial septal aneurysm or eustachian tube (increase possibly recurrent risk) and poss. psychological factors).
Antiplatelet aggregation inhibitors should be continued lifelong after occlusion of PFO.
Reversible Cerebral Vasoconstriction Syndrome
Symptoms
- typically thunderclap headache (in about 65%, sometimes with nuchal onset and then spreading to biparietal), lasting minutes to hours, rarely days; often persistence of a milder headache thereafter
- often accompanied by nausea, photophobia, phonophobia
- depending on severity, neurological deficits, epileptic seizures
Typical triggers
- Sex, pressure, coughing, sneezing, urinating, bathing/showering, swimming, laughing, cannabis, cocaine, excess alcohol
CSL
- Cell count increase and protein increase possible → follow-up after 2 weeks
MRA/CTA/DSA
- typically: diffuse vasoconstriction with (almost complete); increase can still increase over weeks, reversibility within 12 weeks
Diagnostic criteria
- acute and severe headache, often thunderclap headache with/without focal deficits or epileptic seizures
- monophasic course without new symptoms after >4 weeks course
- segmental vasoconstriction in CTA/MRA/DSA
- no aneurysmal SAH
- liquor normal or cell count < 15 or protein < 100 mg/dl
- complete or almost complete normalization of vasoconstriction within 12 weeks
RCVS2 score ≥ 5: PPV 98% NPV 67% sensitivity 94% specificity 86%
Complications
- Convexity SAH (non-aneurysmal)
- ICH
- Ischemias, especially watershed infarcts
- Reversible encephalopathy syndrome
- Brain edema
Therapy: No established treatment; consider: nimodipine, verapamil, magnesium sulfate
Cerebral venous sinus thrombosis
- etiological work-up: infectious, coagulation disorder
- LMWH in therapeutic dosage: e.g. enoxaparin (1mg/kg bw, 2x/d)
- alternatively therapeutic heparinization (aPTT 1.5-2.5x baseline aPTT) particularly in patients with risk of craniectomy; switch to OAC in the course of time
- alternatively Dabigatran can be considered
- continue therapeutic heparinization/LMWH also after occurrence of congestion hemorrhages
- in case of large hemorrhagic infarctions and impending lateral herniation: decompressive craniectomy as early as possible without removal of hematoma or infarcted tissue
- duration of OAC 6 months (except in case of progressive thrombosis at follow-up MRI or known thrombophilia)
- usually examination for coagulation disorders after stopping OAC
CAVE: anticoagulation is contraindicated in Behçet's disease
Secondary prevention
| Etiology | First stroke | Re-Stroke → always repeat or escalate examinations for etiology |
|---|---|---|
| no reason determined (specially no cardiac embolism source, no symptomatic stenosis) | ASS 100mg or Clopidogrel 75mg or ASS+Dipyridamole Ticagrelor (Brilique®) in case of intolerance to the other agents |
Change to Clopidogrel 75mg or ASS+Dipyridamole |
| Initial therapy: in case of TIA or minor stroke within 24h after symptom onset and NIHSS <4, small infarct): 4 weeks ASS 100mg + Clopidogrel 75mg (loading 600mg) when hemorrhagic transformation is excluded and individual bleeding risk is not elevated | ||
| If additionally CHD, peripheral arterial occlusive disease or asymptomatic carotid artery stenosis: rivaroxaban 2x2.5mg + ASA 100mg/d instead of aspirin monotherapy | ||
| non-valvular AF | - DOAC - occurence under sufficient or insufficient OAC => change to DOAC - occurence under DOAC: change substance class (Xa ↔ IIa) - consider atrial appendage closure |
- occurence under sufficient or insufficient OAC => change to DOAC - occurence under DOAC: change substance class (Xa ↔ IIa) - consider atrial appendage closure |
| valvular AF (Def: AF with rheumatic mitral stenosis) | OAC INR 2-3 | 1. optimize dosage if neccessary 2. consider OAC INR 2.5-3.5 3. consider OAC + ASS 100mg |
| symptomatic extracranial carotid stensosis | >50% degree of stenosis: CEA/CAS < 50% with radiologically proven plaque rupture: individual + statin at high dose |
< 50% stenosis with radiologically proven plaque rupture: consider CEA/CAS |
| symptomatic extracranial vertebral artery stensosis | ASS 100mg + 4 weeks Clopidogrel 75mg + statin at high dose Contralateral hypoplasia: consider stenting |
consider stenting |
| symtomatic intracranial stenosis |
ASS 100mg + Clopidogrel 75mg for 3 months, then monotherapy + statin at high dose | ASS 100mg + Clopidogrel 75mg (duration individually) + statin at high dose + consider stenting |
Antiplatelet aggregation therapy after ischemic stroke
- in case of conservative treatment: immediately
- after mechanical EVT: usually immediately with loading (250-500mg ASS or 300-600mg Clopidogrel)
- after IVT, Bridging, Urokinase i.a.: after exclusion of bleeding in 24h control imaging
- in case of imminent space-occupying brain edema neurosurgeons should be involved immediately. If a potential craniectomy is considered, no administration of antiplatelets
Antithrombotic therapy according to cause of transient ischemic attack (TIA)
* Indications for long-term oral anticoagulation include atrial fibrillation, ventricular thrombus, mechanical heart valve, and treatment of venous thromboembolism.
¶ Some experts prefer DAPT based upon observational evidence.
Δ Long-term single-agent antiplatelet therapy using aspirin, clopidogrel, or aspirin-extended-release dipyridamole.
Antithrombotic therapy according to cause of acute ischemic stroke
* Brain and neurovascular imaging, cardiac evaluation, and (for select patients) other laboratory tests. ¶ Indications for long-term oral anticoagulation include atrial fibrillation, ventricular thrombus, mechanical heart valve, and treatment of venous thromboembolism. Δ "Large" infarcts are defined as those that involve more than one-third of the middle cerebral artery territory or more than one-half of the posterior cerebral artery territory based upon neuroimaging with CT or MRI. Though less reliable, large infarct size can also be defined clinically (eg, NIHSS score >15). ◊ Long-term aspirin therapy is alternative (though less effective) if OA contraindicated or refused. § Direct oral anticoagulant agents have a more rapid anticoagulant effect than warfarin, a factor that may influence the choice of agent and timing of OA initiation. ¥ Some experts prefer DAPT, based upon observational evidence. ‡ Long-term single-agent antiplatelet therapy for secondary stroke prevention with aspirin, clopidogrel, or aspirin-extended-release dipyridamole.
Secondary prevention in special situations
Myocardial infarction (sub)acute
- consider DOAC application for 3 months also without thrombus finding, esp. with embolic infarct distribution
- stenting in patients with (D)OAC indication → (D)OAC + clopidogrel (consider DOAC low dose in large infarctions), triple therapy in acute stroke only in exceptional cases (esp. in-stent-thrombosis, stent main stem)
- If AF is indication for (D)OAC: consider atrial appendage closure, afterwards only dual antiplatelet therapy
- STEMI: Coro immediately; NSTEMI: Coro as soon as clopidogrel + ASS or (D)OAC + clopidogrel is possible (depending on indication); Coro immediately in case of severe arrhythmia, hemodynamic instability, persistent pain
Detection of AF or atrial thrombus in patients taking aspirin + clopidogrel due to coronary stent
- DOAC long-term therapy + usually 1 year clopidogrel
- during dual therapy consider (transient) DOAC low dose in dependence on infarct size
Intracardial thrombus
- Ventricular: (D)OAC for 3 months, then control TEE and consider change to antiplatelet therapy
- Atrial appendage thrombus: DOAC therapy life long also without proven AF
Coronary heart disease or peripheral arterial occlusive disease + high risk for ischemic events
- Consider Rivaroxaban 2x2.5mg + ASS 100mg/d
Severe heart failure with severe hypokinesia/akinesia
- No DOAC escept in case of intra cardial thrombus
Infectious Endocarditis
- No antiplatelet therapy/heparin/(D)OAC; if valvular replacement is indicated, early operation seems to be beneficial
Pulmonary embolism
- DOAC, start depends on infarct size; duration: 6 months in case of uniquivocal provocative factors (surgery, immobilization >48h, plaster cast on leg), otherwise long-term therapy;
- PFO occlusion in case of long-term DOAC therapy not indicated, otherwise PFO closure also with low RoPE score
Paraneoplastic Coagulopathy
- LMWH therapeutic dosage (2x/d, not 1x/d) or Edoxaban or Rivaroxaban
Silent strokes
- most frequent incidental finding in CT/MRI (no TIA or stroke suspicious episodes in medical history)
- prevelence depending on cardiovascular risk profile and age (~30% in people aged 70)
- increased stroke risk and severity, risk for dementia, depresssion and subclinical deficites
Definition by MRI
- acute or subacute ischemia (acute diffusion lesion with signal decrease in ADC and without symptoms and without otherwise explanation)
- chronic ischemia:
- T2/FLAIR hyperintense lesion, T1 hypointense lesion non-lacunar
- cerebellar or supratentorieal cortical, or
- supratentorial subcortical >3mm with affection of deep gray matter and without otherwise explana-tion
- lacunar lesion: ≥3mm, not corresponding to enlarged perivasculuar space
- T2/FLAIR hyperintense lesion, T1 hypointense lesion non-lacunar
Definition by CT - cortical defect zone or lacunar lesion
Diagnostics - search for risk factors / complete vessel imaging / ECG monitoring / TTE/TEE
Therapy
- risk factor treatmemt
- ASS with consideration of risk/benefit value
- treatment of blood pressure
- consider treatment of stenosis > 60% of the depending vessel after consideration of risk/benefit value, in case of
- acute ischemia, or
- multiple chronic ischemia in the corresponding vessel territory
Direct oral anticoagulants (DOAC)
- indicated in strokes with evidence of non-valvular AF
- in cerebral venous thrombosis and dissection: phenprocoumon/acenocoumarol or dabigatran
- not recommended in anti-phospholipid-antibody syndrome or valvular AF (valvular: rheumatic mitral stenosis)
- in case of known elevated GIT bleeding risk: preferable lower doses of DOAK especially in patients > 75 years
| Factor II-inhibitor | Factor X-inhibitors | |||
|---|---|---|---|---|
| Dabigatran (Pradaxa®) | Apixaban (Eliquis®) | Rivaroxaban (Xarelto®) | Edoxaban (Roteas®) | |
| CrCl ≥ 50 ml/min |
2 x 150mg (≥ 80 years: 2x110mg) |
2 x 5mg (2 x 2.5mg if two of the following criteria are fullfilled: - ≥80 years - ≤60kg, - creatinine ≥ 133 mol/l |
1 x 20mg | 1 x 60mg (1 x 30mg if bw < 60kg) |
| CrCl 30-49 ml/min |
2 x 110mg | 1 x 15mg | 1 x 30mg | |
| CrCl 15-29 ml/min |
contraindicated | |||
| CrCl <15 ml/min | not recommended | contraindicated | not recommended | |
| Inductors (effect diminished) (bold print: contraindication) |
Rifampicin, St John's wort, carbamazepine |
Rifampicin (edoxaban: dosage reduction not necessary), phenytoin, carbamazepine, phenobarbital, St John's wort | ||
| Inhibitors (effect enhanced) (bold print: contraindication) |
Verampil, ketoconazole, itraconazole, voriconazole, HIV-protease inhibitors, |
Verapamil, ketoconazole, itraconazole, voriconazole, posaconazole, HIV-protease inhibitors | ||
| T1/2 | 12-17h | 9-14h | 5-9h | 10-14h |
| Set off time before surgery | 24h up to 72h in case of large operations 4d with CrCl < 50ml/min |
24h 48h in case of high bleeding risk, renal failure, elderly patients |
||
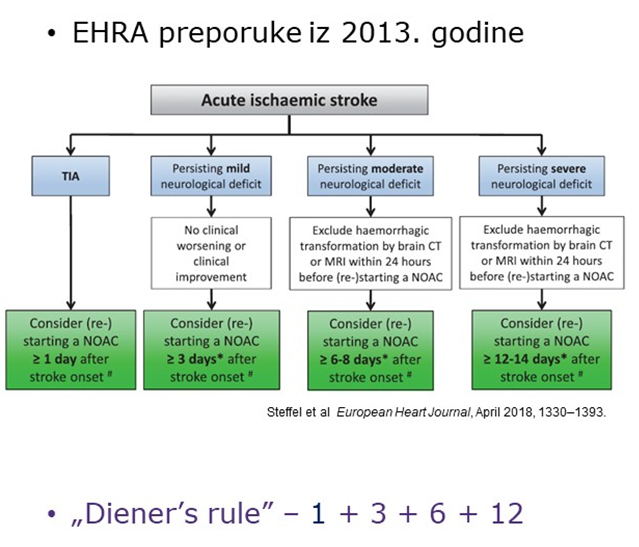
Instructions for the earliest initiation of (D)OAC after ischemic stroke
- CAVE: Exclude hemorrhagic transformation and endocarditis (=contraindications)
- TIA/smallest infarctions: immediate initiation
- Small infarction (≈ <40ml): after 3d (with BG involvement 6d)
- Middle-sized infarction (≈ 40-100ml): after 6d (with BG involvement 9d) after exclusion of hemorrhage
- Large infarction (≈ >100ml): after 12d (with BG involvement 15d) after exclusion of hemorrage
- usually no intermediate antiplatelet therapy until start of (D)OAC
- in case of medication switch: consider transient „dual therapy“ depending on the delayed loss of therapeutic effect depending on T1/2
- highly embolic source of embolism (e.g. mechanical heart valve): consider immediate initiation of a therapeutic heparinization except if infarction is very large or hemorrhagic
- in case of hemorrhagic transformation, initiation usually after 2 weeks (following CT scan)
Arterial hypertension
Secondary arterial hypertension
Look for in the case of resistance to therapy (especially in patient <75 years, normal weight, healthy lifestyle, absence of diabetes mellitus and/or organ damage due to vascular risk factors)
Causes:
- sleep-associated respiratory failure
- primary hyperaldosteronism
- chronic renal failure
- pheochromocytoma
- fibromuscular dysplasia
- coarctation of the aorta
- Cushings syndrome
- Hyperparathyroidism medications (oral contraceptives, sympathomimetic mucosal decongestant therapy, NSAIDs, cyclosporine, erythropoietin, chronic steroid therapy, chemotherapeutic agents)
- drugs (cocaine, amphetamines, anabolic steroids)
Dyslipidemia
The treatment of dyslipidemia and the success of the scheme below requires careful pre-selection of patients. NO mandatory statin therapy is needed, for example, in patients with dissection, confirmed paradoxical embolization, iatrogenic strokes, etc. In these cases, the indication would be with the criteria for primary prevention.
1st choice of statin, increasing dose as long as target value not reached and up to highest tolerated dose.
If target value is not reached:
- Statin+ezetimib and if necessary PCSK9 inhibitors, especially in the case of very high vascular risk
- If necessary, anion exchange resin
- If necessary, fibrates in hypertriglyceridemia
In cases of statin intolerance: switch to another statin, if necessary, ezetimib +/- PCSK9 inhibitors
Strength: rosuvastatin > atorvastatin > simvastatin > pravastatin > fluvastatin
Sleep apnoea syndrome
- Screening with SPG
- Treatment with CPAP/APAP/ASV indicated with
- AHI ≥ 5/h in symptomatic SAS (preexisting sleepiness)
- AHI ≥ 30/h also in asymptomatic SAS
- AHI 5-29/h + relevant general medical indications (e.g. severe heart failure, untreatable arterial hypertension)